Burlington Emergency & Veterinary Specialists
As Vermont’s only specialty and 24/7 emergency animal hospital, Burlington Emergency & Veterinary Specialists (BEVS) provides a level of care you simply won’t find anyplace else in the state.
Specialty & Referral Services
For Pet Parents
For Veterinarians
Veterinary Services
Burlington Emergency & Veterinary Specialists
Is Your Pet Having a Medical Emergency?
Due to the nature of emergency veterinary medicine, wait times may be extended. Please expect a longer wait during high-demand hours, including nights and weekends. We will assess each pet as you arrive and use our triage priority levels to care for the most critically injured or ill pets first.
If you are concerned or unsure if your pet needs emergency care, please call us at (802) 863-2387. If your dog or cat has ingested something poisonous, please call your veterinarian or the 24/7 Animal Poison Control Center at (855) 764-7661 for help immediately. (A consultation fee may apply.)
Our Veterinary Services in Williston, VT
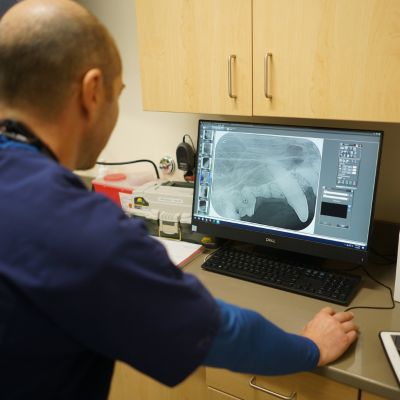
When your pet needs advanced care, you can count on Burlington Emergency and Veterinary Specialists. At BEVS, you and your pet have access to an entire team of specialists, residency-trained veterinarians, and credentialed professionals with the expertise and experience to provide today’s most effective and advanced therapies.

Surgery
Dentistry and Oral Surgery

Internal Medicine

Neurology

Ophthalmology

Meet Our Veterinary Team
Our veterinary team at Burlington Emergency and Veterinary Specialists is committed to providing compassionate and advanced care for your pets. With a diverse group of residency trained specialists, emergency veterinarians, and skilled support staff, we bring a wealth of knowledge and experience to each case. Our team works collaboratively to ensure that your pet receives the highest standard of care, whether it’s a consult with a specialist or a complex emergency. We’re here to support you and your pet every step of the way and are dedicated to their health, comfort, and well-being.

Thank you for your kind words.
See what our clients say about their experiences at our veterinary clinic.